








CES Frequencies and Waveforms
INTRODUCTION
Most clinicians, not usually having much experience or training in electronics engineering, experience confusion about the various waveforms used in cranio-electro stimulation (CES), micro-TENS, micro-current electrotherapy (MET) and so on. This article was written to shed some light on the clinical use of electro-stimulation.
The question often asked is: “What is CES used for and what frequencies/waveforms are involved?”
On the regulatory side, the FDA recognizes CES as a treatment for anxiety, depression (serotonin effect) and pain (endorphin effect). Surprisingly, CES is not regulated for sleep (serotonin effect), even though there are quite a number of favorable sleep studies.
The FDA recognizes only two frequencies for CES: 0.5 Hz and 100 Hz, as these were the two frequencies that were commonly used prior to the FDA’s amendments on medical devices in 1976. CES manufacturers, therefore use these frequencies, as it is makes it easy to get approval (510K pre-market) for marketing within the USA. The negative result of this is that it has stalled research on other frequencies to test their effects, because of the large expense to get approval. However, our CESta and PAL36 with CES use a variety of frequencies in the brain wave range, which is thought to produce mild brain wave entrainment.
NERVE PHYSIOLOGY
A nerve is positively charged on the outside of its membrane (skin) in its normal resting (polarized) state, so a negative electron flow (current) will reverse the resting state of the nerve and activate (depolarize) it. One “treatment” electrode must be negative polarity and the other “reference” must be positive polarity, which provides the return path necessary for stimulation to occur. Typically, the polarity alters back and forth as the electrodes take turns: one providing stimulation, while the other providing the return path and vice versa.
The first thing to understand is that it is only the amperage (known as current) that can cause shock, and therefore, stimulation. However, being that the skin is resistive (it impedes the flow of current), a voltage is needed to push the electrons through to make a current. When using ear clips for CES or small electrodes with Micro-TENS. the electrical resistance through the skin under one electrode, through the body, and out through the skin under the other electrode, is from 10,000 to 40,000 ohms. This resistance depends on skin thickness, dryness, how well the user has wetted the skin, mineral content in the water, and/or if conductive gel is used. It’s fairly common to stimulate both CES and Micro-TENS at 1 to 3 milli-amps (ma). One ma is 1/1000 of an amp, a rather small number. To put this in perspective, a typical wristwatch uses a few microamps of current, while a typical LED indicator light on a so many small electronics items in the marketplace uses 2 to 5 ma of current. The little lights on a CES device typically use quite a bit more power from the battery than the actual stimulation does!
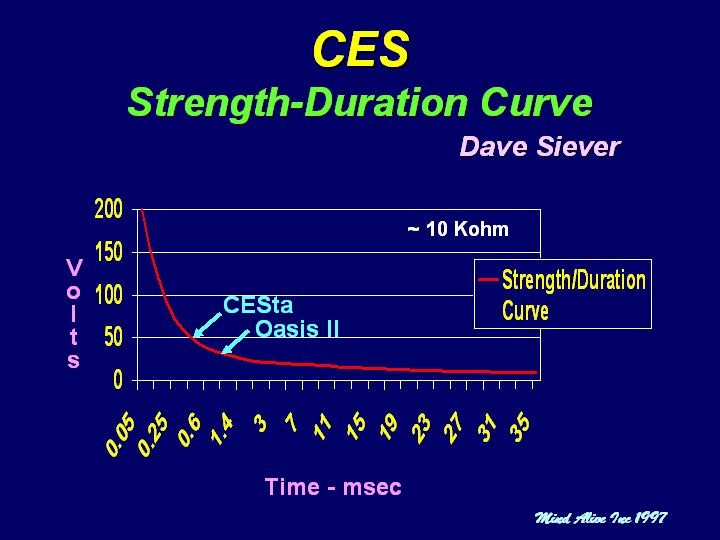
The second thing to understand is that a nerve fires not just from the current flowing through it, but also from the length of time that the current has been flowing through it. This is known as the strength-duration curve. Figure 1 shows that as long as the strength-duration is above the curve, nerve stimulation will occur. Therefore, a very long pulse can exert an effect with very low voltage (and low current). This, in part, is why a 9-volt battery tingles the tongue – because of its good, wet connection, its direct current (DC) and because the current flows indefinitely.
Some devices can deliver pulses beyond 200 volts with very high current but for only 100 microseconds (µsec) which for CES and Micro-TENS is a very short period of time. This approach has a tendency to utilize the capacitance of the body (the ability of the body to store a charge – like sticking a balloon to the wall) and therefore, there is little actual flow of electrons as most of the electrons are just pushed around from within one’s own body. The plus side to this technique is that it’s unlikely to ever burn the earlobes or skin under the electrode. The down side is that if electrodes come in contact with some moist skin on the chest near the heart, it might be dangerous.
The other approach is to use a much lower voltage and current, but for a longer period of time. The plus side to this approach is that it is very safe. The down side is that there is a larger flow of electrons and it can burn/blister the skin. Most CES devices (including Mind Alive CES products) use lower voltage/lower current stimulation. We typically stimulate in the 0.5 to 2 msec range with a maximum voltage of 30 to 40 volts and a maximum current of about 3 ma. Some people have blistered their ears with this, but in all cases, it has been from setting the stimulus to high. Research suggests that a low stimulus is actually more effective than a high stimulus (Arndt’s Law) and the best studies (double blind) show excellent results even when the person cannot feel the stimulation at all! I suggest that the user feel the stimulation just slightly.
Figure 1. Strength-duration curve for nerve stimulation

HOUSEHOLD POWER
To further our understanding of electricity and stimulation, let’s consider household power (what’s in a plug-in). Our household power alternates from positive to negative, back to positive and back to negative 60 times per second, or 60 Hz AC (alternating current). If you should accidentally grab a “hot” power source, you will get a much more severe shock than from an electro-stimulator with the same voltage. This is because at 60 Hz, the “stimulus” is on for about 8 msec (a very long time), then flips polarity for another 8 msec and a lot of current can pass through a person. Due to the long stimulus time, a 60 Hz line shock can really excite nerves and make muscles contract harder than anyone could ever willfully contract their own muscles. As a result, torn muscles and heart attacks are possible, depending on where the hazardous wire contacts the body and the reference or ground. All electricians must, by law, use plastic ladders to prevent shock by accidentally grabbing a hot wire. Table 1 shows the shock hazard at varying currents of 60 AC.
Table 1. 60 Hz AC currents and the human experience
1 ma Perception level
5 ma Mild shock felt, not painful but startling
6-30 ma Painful shock, but able to let go if through the hand
50–150 ma Extreme pain, unable to breathe, severe muscle contractions
1000-4000 ma Mild skin and internal tissue burns. Heart goes into ventrical (1-4 amps) fibrillation (heart flutters but does not pump blood)
5000 ma & up Cardiac arrest
So, it’s not the voltage that does harm, but rather the amperage. Of course, with a low voltage, a better connection is needed to get the amperage through. A high voltage, however, can push a nasty current through the body even if the connection is poor.
I can recall as a teenager spending one summer time in my family’s holiday trailer. The trailer didn’t have a ground wire and one side of the circuit was tied to the aluminum siding while the other side tied to the appliances. This was before the days of polarized plugs, so depending on which way the trailer was plugged into the house power, “hot” could be on the siding. One rainy evening, I came home, all soaked, grabbed the door handle, and with the hot tied to the aluminum siding, I received a pretty good jolt. Fortunately, it wasn’t severe enough to prevent me from opening my hand and pulling it away. I now always touch an unknown shock hazard with the back of my hand. That way, if I do receive a shock, the natural contraction will pull my hand away from the dangerous device – thus ending the shock. The skin on the back of the hand is also much drier and more resistive than the skin on the fingers and palm. Therefore, I will normally feel only a light tingle as a warning to be careful.
The electrical formula is as follows: Volts (V) = Resistance (R) X Amps (A). If a person has 10,000 ohms of skin/body resistance, then the volts needed to push 1 ma through the body will be: (V=R X A). Therefore 10 volts will be needed to push 1 ma of current through (20,000 ohms will need 20 volts and so on).
WAVEFORM
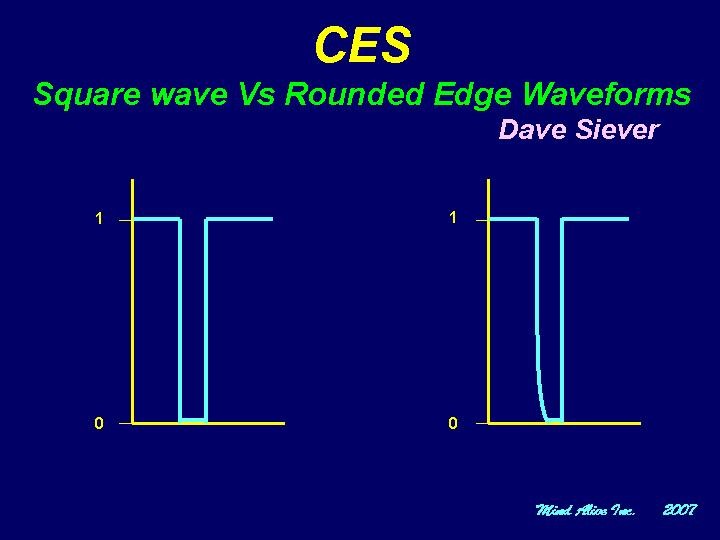
Some manufacturers promote that they use a unique, “special” waveform, which is better than what others use. The truth is that there have been NO comparative studies of different waveforms. Almost all CES and Micro-TENS research has used the simplest waveform to generate, which is a square wave (on and off). Although simple and inexpensive to generate, the down side to a square wave is that the stimulus can really “sting,” especially when the connection isn’t very good. So people with naturally thicker and/or drier skin have more concerns than a person with thinner, moister skin. We have found that by rounding the front end of the pulse, so it doesn’t turn on so fast*, the stinging/burning sensation is reduced by 80% without loss of effectiveness. This increases user compliance, as most people won’t use something that hurts! Figure 2 shows an oscilloscope tracing of our rounded waveform versus a traditional square wave.
Figure 2. Oscilloscope tracing of a square waveform vs a rounded wave.
APPLICATIONS
SLEEP
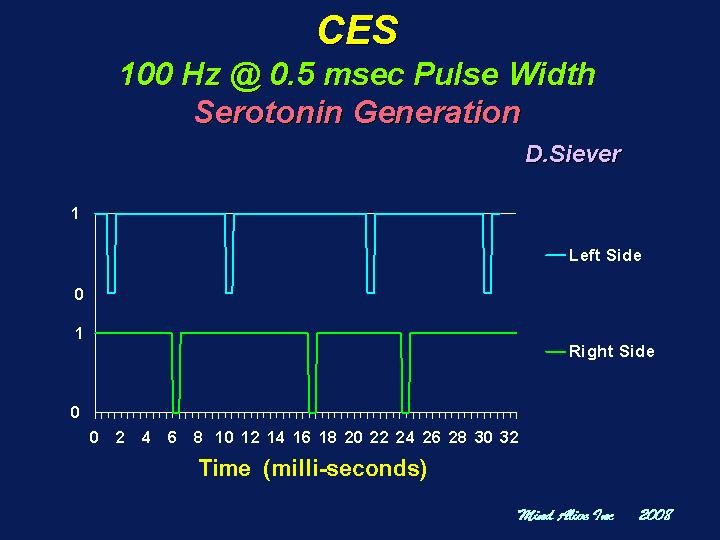
The standard CES approach for sleep is to use a 100 Hz pulse at 0.5 msec in length. Stimulation at 100 Hz is believed to increase serotonin. A 100 Hz frequency means that it occurs every 10 msec. Therefore, with 100 Hz stimulation, there will be a spike every 10 msec. Both left and right are running at 100 Hz, so a spike will occur every 10 msec on both the left and right sides. Being that both sides alternate back and forth, the left and right sides stimulate alternately every 5 msec. This is how the CESta operates. The Oasis, on the other-hand, utilizes randomization where the pulses are delayed or advanced somewhat to reduce habituation.* The randomization from an Oasis, as seen on an oscilloscope, is shown in Figure 3.
Figure 3. Randomized, 100 Hz stimulation
PAIN
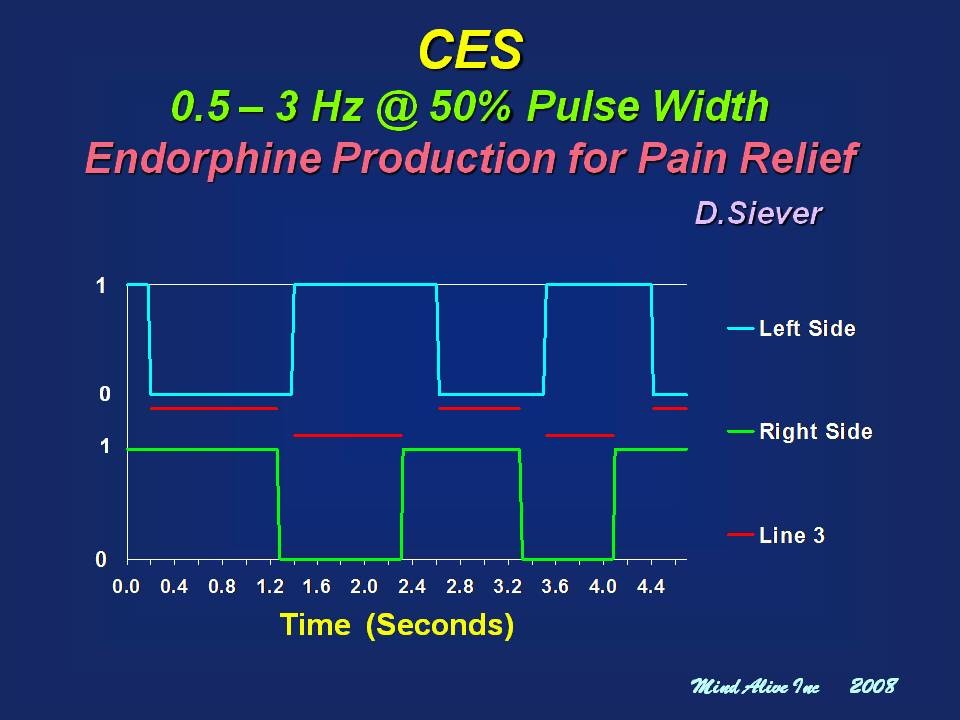
The second official FDA recognized frequency is 0.5 Hz, but instead of producing short pulses, it produces pulses at 50% duty cycle (1/2 of the time on and 1/2 off). Research suggests that this approach produces endorphins and is effective for treating pain. In this case, the current rarely stops flowing, as it does with short pulses. Given that the current is mostly on, the effect is much like tDCS, but across the brain stem. It sure can make some people’s head "spin" or bring about nausea. If this is too much to bear, then using Micro-TENS (short pulse) stimulation will be best. It is less effective, but doesn't produce nausea. Randomized stimulation for both CES and Micro-TENS produces better results.* Notice in the oscilloscope tracing in Figure 4, the red line shows the side where and when stimulation is occurring. Also notice that there are times when both left and right electrodes are positive or negative at the same time and no stimulation occurs (shown by no red line).
Figure 4. 50% Duty Cycle randomized waveform from 0.5 – 3 Hz: endorphin stimulation for reducing perception of pain
MICRO-TENS
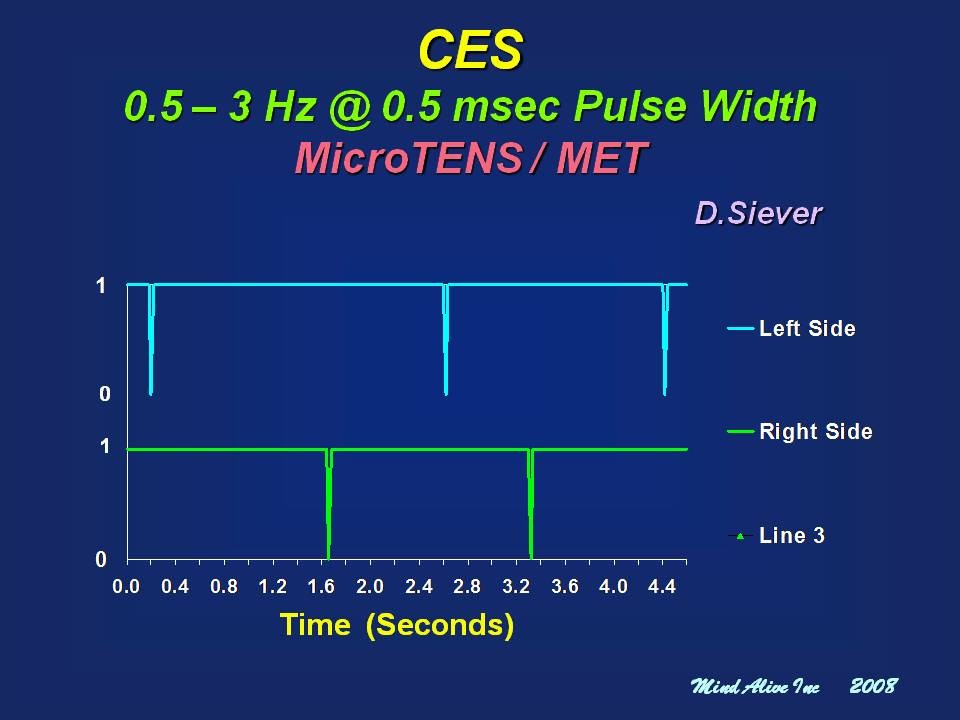
Micro-TENS and MET are meant to be used directly along a muscle to break down knots and fatigue in muscle. It is a slow frequency (like CES for pain), but the pulses are short. The standard protocol has been to use a fixed frequency of 0.5 Hz. However, Heffernan (1997) found that randomized stimulation from 0.5-3 Hz produced superior results. Our PAL36 with CES, the CESta, and Oasis II use dual-randomized low-frequency stimulation. Notice, in Figure 5, how the pulse timing between the left and right sides varies between pulses in accordance with the randomized stimulation.
Figure 5. Randomized 0.5 to 3 Hz stimulation for Micro-TENS
CONCLUSION
There is little in the way of properly explaining stimulation techniques and the reasons for them within CES and Micro-TENS disciplines. With a better understanding of the electrical properties of stimulation, clinicians can prescribe these technologies to their clients with greater confidence and the ability to resolve issues, should they arise.
*The randomizing concepts and rounded wave are patent pending, 2009 by Mind Alive Inc.
Biographical Sketch of Dave Siever
Dave graduated in 1978 as an engineering technologist. He later worked in the Faculty of Dentistry at the University of Alberta designing TMJ Dysfunction diagnostic equipment and research facilities. He organized research projects, taught basic physiology and an advanced TMJ diagnostics course. Dave had noted anxiety issues in many patients suffering with TMJ dysfunction, which lead him to the study of biofeedback.
In 1984, Dave designed his first audio-visual entrainment (AVE) device – the DAVID1 (Digital Audio/Visual Integration Device). Since this time, through his company, Mind Alive Inc., Dave has been researching and refining AVE technology, specifically for use in relaxation, and treating anxiety, depression, PMS, ADD, FMS, SAD, pain, cognitive decline and insomnia. He presents at many conferences and provides training throughout North America and Europe. Dave also designs Cranio-Electro Stimulation (CES), transcranial DC stimulation and biofeedback devices. Dave continues to conduct research and design new products relating to personal growth and wellness.
Email: info@mindalive.com
Copyright 2010, Mind Alive Inc.